|
|
THE EARLY RESOLUTION OF TRAUMAEmersonW.R. during the pre- and perinatal period. Some common forms of aggression are warfare, gang fights, domestic violence, conception through rape, physical or sexual abuse of parents or siblings, annihilative energies, intrauterine toxicities, and/or abortion attempts. Prenates who experience one or more of these aggressive conditions are at risk for manifesting aggression and violence, and the greater the number of conditions, the greater the likelihood of aggression and violence. Adoption Adoption trauma refers to a broad range of painful experiences that are common to adoption. When children are adopted, they are more likely to have experienced some level of abortion trauma--there may have been direct attempts on life, abortion plans with no attempts, or abortion ideations but no plans. All of these are traumatizing to varying degrees. In addition they are likely to have experienced discovery trauma (child unwanted at the time of discovery), conception trauma (child unwanted at time of conception), or psychological toxicity (child exposed to mother's annihilative or ambivalent feelings, or to socio-cultural shame). Adoption trauma has many different levels. The lowest level occurs when parents want their children but reluctantly give them up for adoption because external circumstances dictate. A higher level occurs when parents do not want their children and seriously consider abortion. The highest level occurs when parents are unequivocally opposed to having children, when pregnancies are resented, when abortions, are attempted, when children are put up for adoption, and when children are fostered a number of times. At high risk for aggression are children who experience the severest levels of adoption trauma. Pre- and Perinatal Medical Procedures When prenates experience severe forms of traumatization, as described above, they are also likely to perceive subsequent events in similar contexts. This is especially true when subsequent events are stressful life transitions (such as birth, adolescence, first jobs, new relationships, etc.), and/or when subsequent events are symbolically similar to traumatizing events. For example, if prenates experience prenatal violence, then they are likely to experience life transitions (such as birth) in violent ways. Freud called this process recapitulation. Among other definitions, recapitulation means that prenatal experiences shape how subsequent life experiences are perceived. The following case is an example of a mother who had only limited prenatal traumas, but which nevertheless influenced her baby's perceptions and experiences of the birthing process. The mother was 28 years old, and had never attempted to conceive a child. Her own mother had had difficulty conceiving children, so she was anxious about her ability to conceive. She wanted to have a child, and in spite of being unmarried, conceived a child with her boyfriend, who was also ambivalent. They conceived after much effort, whereupon the boyfriend turned brutal and violent against the mother and her baby (it was later discovered that the boyfiiend's father had been abusive to him during the prenatal period). A series of beatings occurred, after which the mother fled. She spent the remainder of her pregnancy in a distant and safe place, under conditions that were close to "ideal." She was attentive to herself, her body, and to her baby. She meditated daily and earned income from work she did at home. She had an extensive and supportive family system as well as friends, and the remainder of the pregnancy was uneventful in terms of other stresses and traumas. She devoted time to her unborn baby every day, talking and singing to him, and doing bonding exercises. She gave birth at home, and described the birth as short and simple, with no complications. In spite of having a largely positive pregnancy and an easy birth, the early abusive experiences haunted her and her baby. In particular, her baby experienced the birth as very traumatic. (This is not an unusual event, even when mothers describe births as simple and uneventful). This was evident in childhood memories of his third trimester and birth. He experienced his mother's jogging during the third trimester as abusive, saying that his head bounced painfully on his mother's pelvic bones. He experienced the perineal massages (given repeatedly during birth) as intrusive, and the contractions as abusive and violent. He was aware of his mother's physical pain, felt the birth was hurting her, and felt guilty that he could not protect her. In short, all of his birth feelings appeared to be overlays and manifestations of his unresolved abuse traumas from the first trimester. It is important to realize that, even more so than children or adults, prenates perceive and interpret life experiences in terms of past experiences. This is so because prenates do not have sufficient neurological integrity or adequate life experiences to assist in discriminating between current and historical realities. When prenates experience abandonment, rejection, violence, or abuse, as has been described in this paper, they routinely bring these experiences to bear during the birthing process. Amniocentesis needles and chorionic villae catheters are commonly perceived as aggressive, annihilating, and/or rejecting instruments. Anesthetic procedures are often perceived as attempts to disempower or to poison (a reflection of abortion trauma). Augmentations (inductions and "breaking waters") are usually experienced as boundary violations. Forceps and vacuum extractions are often perceived as attempts to control or annihilate. Contractions are often perceived as attempts to annihilate, destroy, or impede. For example, one adult who had been exposed to chemical and mechanical abortion attempts (his mother had taken low-dose cyanide pills and repeatedly pummeled her abdomen and uterus) experienced contractions as attempts to beat him to death, and experienced anesthesia administrations as attempts to poison him. It is vital that medical and obstetrical personnel understand the importance and relevance of pre- and perinatal traumas, and understand that babies are likely to experience the birthing process in terms of prior traumatizations. This means that birth can be very traumatic, simply on the basis of personal history. If this fact were known, then medical interventions could be limited to situations where they were absolutely necessary, or medical interventions could be humanized in a variety of ways. Some useful procedures might be asking the permission of babies to implement procedures and getting responses through the mother's intuition, letting babies know that they might experience pains and discomforts, and empathizing in terms of prior traumas, letting babies know that birth is a difficult transition with the potential for negative and overwhelming feelings and acknowledging babies post-birth emotions as legitimate expressions of a difficult birthing process"all this could help to minimize potential trauma. It is also important to acknowledge the positive aspects of birthing, the wonder and joy that belongs to the birthing process. Few births are entirely difficult, and few are completely free from trauma or pain. We need to acknowledge the whole gamut of human experiences as they unfold during the birthing process. Treatment It is important that pre- and perinatal traumas be treated as early as possible. This is so because, as previously discussed, early traumas shape how subsequent events will be perceived and experienced. If treatment occurs early on, during gestation or the first year, then childhood experiences can be freed from prenatal influences, and children can live their lives unencumbered by the bonds of trauma. The effects of trauma have been described elsewhere (Emerson, 1992, 1994). Unresolved traumas affect the spiritual and psychological development of children. In contrast, children who had no trauma, or whose traumas have been resolved, are clearly unique in the following ways. They are more spiritually evolved, manifest higher levels of human potential, and are developmentally precocious. They exhibit higher self-esteem and intelligence test scores, and they are more empathic, emotionally mature, cooperative, creative, affectionate, loving, focused, and self-aware than untreated and traumatized children (Emerson, 1993). The fact that pre- and perinatal traumas shape how subsequent life events are experienced does not mean that childhood experiences, in and of themselves, are unimportant in terms of human development. On the contrary, childhood experiences are very important in determining and shaping who children will become. It is precisely because childhood experiences are so important that it is vital to free childhood from the bonds of pre- and perinatal trauma. If these traumas can be resolved before childhood, then childhood has the opportunity to be experienced on its own, without traumatic influence from the prenatal period, and without the defensive forces that inhibit feelings of safety, security, and growth. Furthermore, children can be freed to exhibit and manifest their own unique human potential, to utilize their own inherent levels of intelligence, and to, become themselves, unencumbered by prior traumas. In addition to these benefits, society can be freed from the increasing burden of aggression and violence. According to statistics reported at the 1995 APPPAH Congress, violence and aggression are on the rise, and are reaching epidemic proportions. Therapists who specialize in anger resolution report that about one client in five carries a significant degree of anger and rage. Aggression and violence are on the rise, and are extremely costly in terms of human lives, in terms of financial and budgetary considerations (prisons, jails, and law enforcement are very costly, and deprive our school systems of needed finances), and in terms of the safe and efficient functioning of our institutions. These violent feelings are directed toward self and others, and are very difficult to resolve for the following reasons. First of all, most therapists do not realize that anger and rage, at their deepest levels, are caused by pre- and perinatal traumas, and are related to perinatal bonding deficits. Secondly, most clinicians fail to realize that anger and rage cannot be resolved solely by talking therapies. Instead, anger and rage require physical and emotional release. Third, anger and rage are inextricably intertwined with low self-esteem, shame, guilt, disempowerment, and forgiveness. These concepts need to be understood and recognized in the treatment of aggressive disorders. Finally, the ultimate resolution of rage and anger requires that relevant pre- and perinatal traumas be uncovered, encountered, catharted, repatterned, and integrated into consciousness. Additional aspects of treatment should include opportunities for re-bonding, i.e., for bonding in ways that were impossible at the time of traumatization, or bonding in ways that were inhibited by unresolved traumas. The Association for Pre- and Perinatal Psychology and Health, the International Primal Association, The Star Foundation, and Emerson Training Seminars have personnel and lists of professionals who do such work. References Bloch, G. (1985). Body & Self. Elements of Human Biology, Behavior, and Health. Los Altos, CA: William Kaufmann, Inc. De Zulueta, F. (1993). From Pain to Violence. London: Whurr Publishers. Emerson, W. (1994). Trauma Impacts: Audio taped presentations. Seattle 1992, Petaluma 1992, and March 1993. Emerson Training Seminars. Emerson, W. (1995a). "The Vulnerable Prenate." Paper presented to the APPPAH Congress, San Francisco. Available on audio tape from Sounds True (303) 449-6229. Emerson, W. (1993). "Treatment Outcomes," Petaluma, CA: Emerson Training Seminars. Emerson, W. (1995/1996). Treating Birth Trauma During Infancy. A series of five videos. Available from Emerson Training Seminars, Petaluma, CA: (707) 763-7024. Laing, R. D. (1976). The Facts of Life. New York: Pantheon Books. Magid, K., and McKelvey, C. (1988). High Risk: Children Without a Conscience. New York: Bantam Books. Editor's Note: Readers may be interested in an earlier article by Dr. Emerson, "Psychotherapy with Infants and Children" published in the Pre- & Perinatal Psychology Journal Vol 3(3), Spring 1989. This article includes drawings made by children in the course of treatment. The author invites email addressed to starvapor@aol.com. The Mind-Body Spirit Connection: Ancient and Modern Healing Strategies for a Traumatic Birth and the Sick Newborn Ruth D. Rice, R.N., Ph.D. Reprinted from Volume 1 (1), 1986 (Fall) Address correspondance to the author at: 6401 Bay Street #8122, Emeryville, CA 94608 Let us talk of healing. The ancient wisdoms teach that all worlds exist now--the past, the present, and the future--all co-existing simultaneously. Man invents nothing. He merely discovers, interprets, and reports what already exists in nature. Many medical doctors believe that it is really nature that heals, not the doctor or the drug, and that medicine merely assists the patients to heal themselves. The traditions of both wisdom healing and physical medicine can trace their origins back 2600 years to the third Egyptian dynasty of King Zoser, and that master healer-physician, Imhotep. Throughout the flow of human civilization, in Greece, China, Persia, Africa, and India, wisdom healing and physical medicine were not separated. True healing treated man as a whole, as spirit, mind, and body. This concept is epitomized in the 3,000 year old Oriental system of Ayurvedic medicine, which not only incorporates over 2000 medicinal herbs and minerals, but also includes surgery, psychoanalysis, and the cleaning of man's subtle energy-body.1 The great healer-physicians of history, including Hippocrates, Avicenna, Paracelsus, and Galen, all recognized that man is far more than a mere physical body and that any attempt to truly heal by treating the body alone is partial and incomplete. Paracelsus, as a healer-physican, overshadowed his medical contemporaries and set the standard for European medicine for many centu ries. He is credited with having founded the sympathetic system of medicine, wherein everything which occupies space-all bodies, plants, minerals, heavenly bodies--influence man by means of subtle ener gies. He stated that "the ultimate cause of illness is a weakness of the spirit" and he advised his fellow physicians to search within themselves for spiritual insight to heal their patients. Hippocrates also held to the practice of healing the spiritual as well as the physical parts of his patient's illness. The birthplace of Hippocrates, the island of Coz, was reputed to have special healing powers, a curative vibration, inherent in the earth and in the surrounding atmosphere. A word must be said about Shamanism. Dr. Michael Harner states that Shamanism represents the most widespread and ancient system of mind-body healing known to humanity. He states that the methods are at least 20,000 or 30,000 years old. The Shaman is able "to transcend the human condition and pass freely back and forth through the different cosmological planes." Shamanism flourished in the ancient cultures that lacked the technology of modern medicine.2 Now on the eve of this twenty-first Century, we stand upon the shoulder of centuries of ancient healing tradition, peering still further into the bio-psychic evolution of our species. What possibilities do holistic health and consciousness research hold for our expanded awareness as healers? Some of the most influential present day research has been done by Dr. Victor Beasley and Dr. Christopher Hill in connection with Chakra functions, energy vibrations, and healing. Basically, they found that "human consciousness is a product of light and that an in dividual's perception of the world is determined by how cosmic light, breaking up the stars' and the sun's undifferentiated white light into the seven color spectrum of the rainbow. Thus light, or cosmic energy, becomes both the creator and the conditioner of the human consciousness and health. The situation is somewhat analogous to holographic laser technology wherein coherent light from a single source is divided into two separate beams, passed and refracted through certain filters, and eventually recombined as a standing wave form which creates an image we call a hologram. Human consciousness then is a hologram created by cosmic light-energy." Hence, all energy from light, sound, color, and all substance becomes increasingly important to the well-being of the individual and has relevance for modern day healing strategies.3 Our hospitals, like our prisons, are made of concrete and steel, are for the most part void of natural light, color, and sound, and contain little, if any, negative-ion charged air. Individuals placed in solitary confinement suffer severe disturbances in consciousness, and we create a similar kind of deprivating environment when we place our babies in Neonatal Intensive Care. Both ancient and modern medicine are well aware that sudden, intense, or prolonged stress is known to predispose one to disease and to cause a breakdown in the physical cells and in tissues. Stress tightens the body, blocks the chakras, and interferes with the free flow of energy, both from within and from without. It is well known in the present day Eastern and Western medicine that relaxation is a primary requisite for healing and is a major component of any healing strategy. This premise was also accepted in ancient healing. Relaxation for healing was induced in ancient Africa by placing the patient in a circle of drummers. The monotonous, continuous drumming brought relaxation and subsequently an altered state of consciousness. In Egypt, China, and India, drums, chants, music, bells, water, movement, and meditation was used to create deep states of relaxation so that healing could take place. A few hospitals today have innovative provisions for reducing stress in the adult and older child, yet virtually no hospital has considered stress reduction for the NICU. Unfortunately, much of the stress reduction being done in modern medicine has to do with drug therapy-relaxants and tranquilizer-chemicals which act on the nervous system as depressants. If our earliest beginning is in a stress-free womb, life is easy and progressive. If, however, the mother smokes, drinks, has poor nutrition, or has a great deal of anxiety and unhappiness, the intrauterine environment is not a healthy one, and the fetus and consequently birth is adversely affected. Drs. Thomas Verny,4 Stanislav Grof,5 and others have awakened us to the developing consciousness of the fetus, of the energy vibrations being transmitted not only through the maternal system, but also from the external environment. Let us consider birth. The process has moved from natural, primitive environments to modern, technological settings of sterile stainless steel. We are connected to machines that interfere with the natural progression of birth. We use machines to make diagnoses that we don't trust our wisdom to make. A particular care is the routine use of the fetal monitor, which many feel has contributed to our high rate of cesareans due to inaccurate reading of the infant's condition. We justify the whole sale use of sedatives, artifical hormones to stimulate labor, amniotomy, epidurals and other anesthesia, episiotomies, forceps, and the controversial anmiocentesis and ultrasound procedures. Much of this medical intervention becomes iatrogenic and toxifies both mother and infant. In this strange, technological, and unnatural setting, both mother and in fant become stressed. In the earliest stages after birth, the infant is in a state of consciousness that is all sensation. He has no capability for thought or reason, reflection, or judgment. He is more vulnerable to his experience than an adult, for he has no precedent, no frame or reference with which to qualify or to understand his impressions and sensations. In the womb, the infant had all his expectations fulfilled. Nothing has prepared him to be alone and even less, left alone to cry. Nothing has prepared him for a pin. He becomes confused, his crying--the only language he knows--doesn't bring relief. His sense of rightness or essential goodness about his universe and the people in it becomes distorted. He becomes distrustful, confused, and frightened away from his mother's body. He is in a state of stress and pain. Jean Liedloff in The Continuum Concept,6 writes "the infant (like the Guru) lives in the eternal now. The infant in arms (like the Guru) lives in a state of bliss. The infant out of arms is in a state of longing in the bleakness of an empty universe." As our technology increases and the biological survival of the child becomes paramount, the possibilities for stress increase. Even to the most sophisticated observer, a walk through an NICU reveals an environment of space-age technology of chemical and medical interventions. The injections, gavage, blood taking, insertions of catheters and needles, and the use of ventilators are clearly stressful at best and create torturous emotional conditions for the infant. We see infants with scarred and deformed heels from repeated heel sticks, with deformed and sometimes irreparable damage to the palate and upper lip from feed ing tubes, many left in long past the time when the infant could nurse from a nipple. Surely the most frightening and agonizing procedure for the sick infant is the injection of curare to paralyze them for the use of a new space-age jet ventilator. Stress and anxiety increases the MAO levels, and the entire immune system is disturbed. Many chemical and mechanical treatments are continued long after their value as diagnostic or life-saving agents have passed. The complications that almost routinely develop are often more insidious than the original condition. If these conditions existed anywhere but in a hospital, we would be charged with child abuse. And abuse it is--of the cruelest and most frustrating kind. We save lives, but in the process, we frequently are damaging the quality of the emotional and spiritual essence of the infant. The effect of this trauma can last a lifetime. One of the most frequent iatrogenic conditions we see is in newborn jaundice. Although phototherapy with bilirubin lights has been used for more than 20 years, it is still not clear which babies should be put under the lights, for how long, what wattage the lights should be, how effective the process is, and how extensive the side effects are, especially long term effects. Speck stated that phototherapy "may alter the DNA of human cells and may be a carcinogenic hazard." The infant is often separated 23 out of the 24 hours from his mother, sometimes for a week or two. The lights, which are blue and white fluorescent, also have been known to affect the nursing staff with discomfort and vertigo. The atmosphere in the NICU is charged with positive ions. Energy from natural sources for babies and nurses is blocked. The burnout rate among personnel is higher than in any other unit of the hospital. Hippocrates said, "first let us do no harm." The best intentioned physicians sometimes prescribe drugs or treatments which do more harm to toxify their patient's system than to correct the cause of the illness. This is not always the doctor's fault, who may be acting properly and practicing state of the art medicine. The problem lies more with conventional drug and treatment therapy as an incomplete approach to healing. In every NICU we see infants lying passively. Many do not cry. Those who do, have weak, little wails of protest that for the most part go unanswered. The "inhibition of action" behavior was first discussed in 1952 to describe the submissive behavioral pattern, a pathogenic state, that re sults when the organism can not respond to stress and does not generate noradrenaline and cortisol in the body.7 Noradrenaline sets the system in action for fight or flight. The hypothalamus is activated and kept in an overload condition. Cortisol triggers the inhibition of action and depresses the immune system and so a vicious cycle is set in motion. When this kind of "lockjaw" condi tion exists even for a short time, we begin to see damage. The inhibition of action syndrome produces apnea, cardiovascular, gastrointestinal, and upper respiratory damage. It produces emotional damage in supressed energy, lack of trust, and an inability to form attachments and bonds. The infant becomes tactile defensive, pathologically passive, with rigid musculature or lack of muscle tone. Thought processes become abberant because of pain and a sense of futility and abandonment. Dr. Walter Hess produced the changes associated with the fight/flight response by stimulating an area within the hypothalamus of a cat. By stimulating another area of the hypothalamus, another response was produced whose physiologic changes were similar to those produced during the process of meditation or deep relaxation. This response is similiar to an altered state of consciousness or an alpha wave state. Hess termed this reaction "the trophotrophic response" and described it as a protec tive mechanism against overstress, which promotes healing processes. Endorphines are produced and a sense of well being occurs.8 There is a spate of modern day research which shows that patients who receive relaxation techniques have lower levels of adrenaline, lower and more stable blood pressures, and slower and more regular heart rates. Research with premature infants shows there is a greater output of somatotrophin growth hormone, indicating increased myelination, when tactile and vestibular stimulation is provided them soon after birth.9 Bovard found reduced pituitary-adrenal and sympathetic-adrenal responses and found that anabolic process were stimulated when gentle touch was provided.10 Weinberg's classic study found there was less output of cortisosterone when the organism was under stress if there had been gentle stroking and touching prior to the onset of stress.11 Ancient healing wisdoms and shamans knew of this protective healing mechanism and attempted to elicit the responses in their patients. The healing response can be produced in the organism through deep relaxation or meditative states with measures such as rhythmic movement, gentle stroking, massage, affectionate touch, muted monotonous sounds, certain music, colors, and water, aided with negative-ion charged air. Ancient healing was frequently conducted in the out-of-doors, in mild, warm sunlight or near the ocean. To elicit relaxation and healing responses, mothers in Pithiviers, France, Caracas, Venezuela, and a few other places in the world, are being given the freedom to move about during their labor to assume any position they choose, and to have the people to whom they feel emotionally close with them. In these birthing centers medical intervention is kept to a prudent minimum and great attention is given to reducing stress. Music of the mother's choice can be played. Soft, muted colors surround her in her visual environment. The energy from the color is assimilated and is used to alleviate pain. Growing green plants are placed in the room to provide plant energy. Natural lighting should be used. Artificial lighting should be dimmed or candles used. Some women may like the smell of incense burning. The mother is given nourishing food or drink to sustain her physical energy. She is surrounded by other tender and caring women to comfort and assist her to give birth in a natural, safe, and facilitating position. Top priority is given to the quality of the physical, mental and emotional setting. Mothers are encouraged to be open and receptive to their natural and instinctive impulses. They are free to cry, to scream, or to make any noises or sounds that comfort them or express their feelings. When we close off our sounds, we tighten muscles and obstruct feelings. If a mother chooses, she can give birth in a tub of warm water. In these places, medical technology is applied only when needed. There is no interference in the normal sequence of labor, birth, and the post-birth period. The unit of mother, father, and infant is kept intact. Above all, the attendants permitted at this miraculous event must be sensitive, calm, confident, and loving. They must also be without ego and lend their positive, healing energies to the birth process. Much has been written about the healing power of a loving caregiver. As a baby emerges, the mother responds instinctively and puts the baby to breast. It also seems instinctive for her to want to return her baby to moisture, to water. A tub of warm water is provided for her to immerse the baby. A mother's healing, and that of the baby, is largely dependent on their symbiotic relationship, expecially if birth is traumatic. Mother and baby must remain together for physiological as well as psychological healing and nurturance. Dr. Marshall Klaus has stated that the sensory interaction of mother and infant, the transfer of energies from one to the other produces hormones and enzymes that promote healing homeostasis in both.12 Touch is vital to the newborn. Throughout history, mothers have known that the survival of the species depended on their close physical contact with their baby. Research indicates that the infant is more responsive to touch within the first 5 days than to any other form of stimulation. Other tactile healing measures such as laying the baby on a lamb's wool skin can be used; those from New Zealand have been researched and seem to have special healing properties.l3 Only natu ral, soft fibers should be used next to the infant's skin. Frequent immersion in warm gentle moving water is very healing. The benefits of water therapy are multiple and many infants in NICU could be placed in small tubs of water for relaxation. Visual healing strategies can be used by presenting colors on cards or swatches of cloth with all the rainbow colors. It is known that the cones, the light receptor cells in the eye that give color vision, are not well enough developed in the newborn to see color, so bright reds, blues, purples, and greens could be used for energy vibrations. Hanging crystals for sun-ray energy vibrations would also be stimulating. Auditory healing strategies such as monotonous, rhythmic sounds are very helpful. Cassette tapes can be played to the infant that provide many different kinds of healing energies. Sounds of the ocean or soft drum beats such as the kind Dr. Michael Harner recorded can provide deep relaxing states.14 A chanting tape produced by Brother Charles has been found to be very relaxing and almost hypnotic. The intrauterine sounds have been researched in many nurseries and have been found to create soothing, comforting effects in newborns. Music of Bach, Kitaro, Halpern, Georgia Kelly, and many other composers provide healing through auditory senses. Vestibular healing measures can be provided by the use of cradles, hammocks, rocking, and other forms of gentle and rhythmic movement. Our effort here is to create a healing sensory environment which will relax and sooth the infant so that emotional and physical healing can take place. The healing energies described here are designed to open the healing channels in the infant and to provide healing energy vibra tions to counteract the detrimental influences of the NICU. This kind of a sensory stimulation is not to be confused with the mental and motor stimulation which is used in many newborn and intensive care nurseries today, and is designed to activate and stimulate the infant's physical development. The kind of healing strategies described here are to provide deep relaxation, to elicit the trophotrophic response, and to promote healing on all levels for the infant. In 1979, Dr. Victor Beasley wrote that "healing is no longer something that occurs exclusively in man's physical body, as determined by the presence or absence of clinically detectable symptoms, pain, or other somatic disease. Healing attempts to tune the entire being into a harmonious whole. This is something we and ancient medicine have long known in theory. Now we are challenged to give practical manifestation to this knowledge. Healing in its essence is a spiritual-soul impulse operating in the worlds of matter, for in the ultimate sense, the patient, not the physician, heals himself through contact with the higher forces of his own cosmic-governed consciousness, whether or not he is aware that such contact has been made. This is Nature's reality.''16 We must strip away culteral mislearnings in order to discover our instinctual selves, to discover creative, spontaneous rhythms of healing that have abounded in our Universe since the beginning of time, to trust our innate wisdom, to trust our body's signals, to trust the prudent use of technology and pharmacology, knowing that in its extravagant use, we can go astray and create harm. We must learn to be patient with the body's healing time schedule, to believe intently that we, as caregivers, have unlimited and untapped healing power to transmit through natural and simple ways to the mother and her infant to enable them to mobilize their own healing energies. References 1. Beasley, V.: Subtle-Body Healing, Boulder Creek, California, 1979, University of the Trees Press. 2. Harner, M.: The Way of the Shaman, New York, 1980, Bantam Books, p. 52. 3. Beasley, V.: Subtle-Body Healing, Boulder Creek, California, 1979, University of the Trees Press. 4. Verny, T.: The Secret Life of the Unborn Child, New York, 1981, Simon and Shuster. 5. Grof, S.: Realms of the Human Unconscious, New York, 1976 Dutton. 6. Liedloff, J.: The Continuum Concept, 1977, Warner Books, New York, p. 48. 7. Odent, M.: Birth Reborn, New York, 1984 Panthenon. 8. Benson, H.: The Relaxation Response, New York, 1975, Avon Books 9. Rice, R.: Neurophysiological development in premature infants following stimulation, Developmental Psychology 13(1) 1977 pp. 69-76. 10. Bovard, E.: The effects of early handling on viability of the albino rat, Psychological Review 69(5), 1958, pp. 257-269. 11. Weininger, O.: Physiological damage under stress as a function of early experlence, Science 119, 1954, pp. 285-286. 12. Klaus, M.: Maternal-infant bonding, Saint Louis, 1976, The C. V. Mosby. 13. Rosnick, Y.: Health Care Products, P.O. Box 26221, Denver, Colorado 80226. 14. Harner, M.: Drumming for the Shamanic Journey, Dolphin Tapes, P.O. Box 71 Big Sur, California 93920. 15. Brother Charles: The Ecstasy of Peace, A Thousand Names of God as Mother Shrine of the Heart, P.O. Box 8091, Charlottesville, Virginia 22906. 16. Beasley, V.: Your Electro-Vibratory Body, Boulder Creek, California, 1978, University of the Trees Press.
 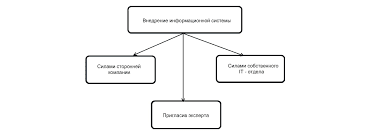 Что делает отдел по эксплуатации и сопровождению ИС? Отвечает за сохранность данных (расписания копирования, копирование и пр.)...  ЧТО ПРОИСХОДИТ ВО ВЗРОСЛОЙ ЖИЗНИ? Если вы все еще «неправильно» связаны с матерью, вы избегаете отделения и независимого взрослого существования...  ЧТО ПРОИСХОДИТ, КОГДА МЫ ССОРИМСЯ Не понимая различий, существующих между мужчинами и женщинами, очень легко довести дело до ссоры...  Что будет с Землей, если ось ее сместится на 6666 км? Что будет с Землей? - задался я вопросом... Не нашли то, что искали? Воспользуйтесь поиском гугл на сайте:
|