|
|
Нейро-биологические аспекты дыханияДыхание можно описать как выдувание мехов «огня Жизни». Любой, кто «постоянно и успешно» занимался Пранайамой в течение довольно длительного времени, подтвердит положительное физическое и психо-духовное воздействие этой практики. Действительно, как говорит Патанжали «Пранайама – это важный компонент Аштанга йоги, предписанной тем, кто стремится к духовной жизни через Раджа йогу». Хатхайога прадипика считает эту практику важным шагом в восхождении к Раджайоге. Прежде, чем говорить о нейробиологии Пранайамы, было бы полезно остановиться на значении и важности самого слова. Буквально оно означает «отлив и прилив праны». Слово «прана» нелегко перевести с санскрита на английский. Оно скорее представляет всеобъемлющее понятие энергетического интегрирующего потока, который плетет Жизнь из «Пракрити». Именно здесь, в воздушных потоках нашего дыхания, а также в потоке биоэлектричества через мириады аксонов и дендритов миллиардов нервных клеток наполняется энергией и интегрируется наше Существо. Именно в энергетике десятков тысяч сбалансированных биохимических реакций, происходящих внутри клеток и через клеточные барьеры, ткани и системы органов рождается удивительное явление – Жизнь. Слово «Пранайама» скорее означает «отлив и прилив» этой «Энергии, дающей жизнь». На мой взгляд трудно сочетать очевидную несовместимость всеобъемлющего понятия «Прана» с одной стороны и приземленного акта дыхания и связанных с ним упражнений, которые слово «Пранайама» представляет в обиходном понимании! Хотя вдыхание кислорода и выдыхание углекислого газа являются центральными в физиологии дыхания, важно понимать, что есть другие жизненно важные нейробиологические показатели этой физиологии – ритмическое дыхательное движение, которое порождается в кардиореспираторном центре ретикулярной формации ствола мозга. Сейчас признается тот факт, что ретикулярная формация ствола мозга и химикоэлектрическое влияние, индуцируемое им, подают на все важные корковые и подкорковые нервные структуры то, что структурирует «Человеческое Сознание». Как мы знаем сегодня благодаря использованию сложных новейших технологий, таких как функциональный ЯМР и ПЭТ (эмиссионная позитронная томография), сознательная концентрация на любой деятельности тела усиливает кровоснабжение и обменные процессы в соответствующей части мозга, которая представляет/контролирует эту деятельность. Основываясь на этом факте, можно заключить, что ритмичное дыхание и его варианты, как предписано в различных практиках Пранайамы, с полной сознательной концентрацией на процессе может нейробиологически влиять на ретикулярную формацию ствола мозга и регулировать сознательную деятельность человека. Сегодня мы также понимаем сложные пути, по которым восходящее влияние ретикулярной формации влияет на все ключевые составляющие человеческого сознания. В свете этих знаний о нейробиологических коррелятах дыхания и его связи с нервным субстратом человеческого сознания, легко понять, почему практика Пранайамы является ключевым элементом Аштанга йоги «Духовной саданы», предписываемой для естественного расширения человеческого сознания.
B. N. Gangadhar, Addl. Professor of Psychiatry N. Janakiramaiah, Professor of Psychiatry, National Institute of Mental Health and Neurosciences, Bangalore Summary Depression is the most common psychiatric disorder. Available effective treatments have certain limitations. Role of traditional methods for treating depression has come under investigation. Sudarshan Kriya Yoga (SKY) is one such traditional approach gaining attention. The yoga research group at NIMHANS has conducted clinical trials of SKY in depression. Results indicate that SKY has significant antidepressant effects and also SKY compares favorably with imipramine - an established antidepressant medication. Following successful treatment with SKY, a neurophysiological 'correction' occurred. P300 event related potential's amplitude was smaller during depression and became 'normal' after treatment with SKY. SKY produced specific neurohormonal responses. Acutely following SKY plasma levels of prolactin were elevated but not that of cortisol. Regular practice of SKY (for two weeks) even lowered plasma cortisol. Role for SKY in the routine treatment of depression deserves to be explored. Mechanisms of therapeutic action of SKY also merit investigation. Depressive Disorder Depression is the most prevalent among mental disorders in the community. Today, an estimated 350 million people suffer from depression worldwide. It will be the number-two cause of "lost years of healthy life" in future years, next to ischaemic heart disease. It also is a condition that contributes to most loss of productive human days adding to personal, psychosocial and economic costs1. WHO global burden study identifies depression as one of the four most disabling illnesses in the world2. High rates of recurrences, chronicity and associated medical &/or psychiatric co-morbidity add to this disability3. Both directly and indirectly it also contributes to mortality; suicide and myocardial infarctions. Prompt recognition and effective treatment of depression hence are top-priority public health issues. Feelings of sadness, loss of interest, psychomotor retardation, low self-esteem including suicidal ideas/plans and vegetative symptoms (loss of appetite, loss of weight, sleeplessness, loss of libido and autonomicity of mood) characterize depressive disorder4. Major depression is typically a recurring disorder. Starting in half the subjects before 40 years, it tends to have frequent recurrences as age advances. The prevalence rates are hence highest in middle-aged. When severe, psychotic Ihsymptoms color the illness. Dysthymic disorder is other chronic, milder but more prevalent condition. Depression is also a phase in the cyclical bipolar disorder, the bipolar depression. Depression coexists with several primary psychiatric conditions causing a pathoplastic influence on them. Depression is also a presenting/coexisting feature of several medical conditions. This is either a biological or the psychological consequence of the medical condition. Treating depression Biological treatments for depression include electro convulsive therapy (ECT) and medications. Other therapies include psychological (psychotherapies, behavior therapies, cognitive therapy, etc.) and yogic. ECT was the first and most effective treatment known for depression. In the second half of 20th century potent antidepressant medications were introduced. Notable among them are the mono amino oxidase inhibitors (MAOI), tricyclic antidepressants (TCA) and the other newer antidepressants. By this time the standards of treatment trials too had improved remarkably. All these drugs proved successful in rigorous, controlled, prospective, double blind trials. ECT too was tested in depression using these standards. The efficacy of ECT was confirmed in many double blind, sham-ECT controlled trials. In its status report the Royal College of Psychiatrists5 noted that the role of ECT in depression is 'incontrovertible'. Interest in ECT increased with drug-nonresponsiveness in a sizeable proportion of depressives. Trials on ECT confirmed its effectiveness in patients who failed to respond to drugs. Yet, a proportion of patients have either no response or unsatisfactory response to the available therapies. The 'drug' therapies have other limitations; their side effects and a lag in onset of antidepressant effect. Research was hence focused on developing side-effect-free and fast-acting drugs, with no breakthrough. Refinements have also occurred in ECT practice; modification, optimizing the stimulus standards, lowering the ECT frequency are a few to note. These treatments make the patient feel that the improvement occurred due to the drugs and not by his/her own 'mental strength'. This may indirectly add to the low self-esteem, which is already haunting the patient. This leads us to the 'heel-thyself psychological treatments. A good number of psychotherapeutic approaches are in use in different forms and with varying success. There are of course some limitations. These therapies are culture-based and lack universal standards. There is difficulty in conducting controlled trials, double blind in particular, to evaluate these therapies. Severely depressed patients or those with psychotic/melancholic symptoms may not be suitable for psychotherapies. Patients with milder/chronic depression, which is determined by individual's personality or psychosocial situations, can be treated by this approach. Lack of trained personnel, longer contact desired and hence, increased cost of these treatments have prompted search for alternative treatments for this widely prevalent disorder. Yogic practice could be a potential alternative. Yoga is a major Indian tradition, which is relevant to medicine and psychiatry. According to Patanjali's Yogasutras, Yoga aims at "the calming of the operations of consciousness". Chronic anxiety and stress are implicated in depression. Stress-reduction procedures such as Yoga can therefore be expected to reduce depression. Sudarshan Kriya Yoga (SKY) Sudarshan Kriya is an innovative yoga procedure developed and popularized by Sri Sri RaviShankar from Bangalore, India. It could be useful in treating depression for two reasons: 1. Several individuals attending the Sudarshan Kriya courses for stress management conducted by the Art-of Living foundation, reported relief from negative emotions, insomnia and fatigue. It had significant neurobiological effects; it elicited high amplitude discharges in the EEG of regular practitioners6. Hence, using contemporary scientific methods we examined its antidepressant effects. Clinical Trials on SKY We have conducted three clinical studies at the National Institute of Mental Health and Neurosciences (NIMHANS) Bangalore. We have omitted the initial philosophical, inspirational briefing to exclude cognitive/suggestion elements and minimize activation of positive expectations. This was 'abbreviation', Sudarsha Kriya Yoga (SKY), was done for the research purpose of operationalizing the procedure to specific/replicable elements as for as possible. We have documented this (SKY) in a videocassette that is available for reference and education7. SKY has three sequential breathing components interspersed with normal breathing: Ujjayi (slow breathing, 2-3/min), Bhastrika (rapid, forced expiration, 20-30 cycles/min), and cyclical breathing (going through increasing frequencies of 20-40, 40-60, and 60-80 cycles/min). All these rhythmic breathing components are practiced while sitting with eyes closed and awareness focused on incoming and outgoing breath, over a period of about 30 minutes. A state of relaxed I sleepiness descends by the end of the last round of cyclical i breathing and the procedure closes with a period of about 10- 1 15 minutes of Yoga Nidra (tranquil state) in supine position. | The entire session lasts for about 45 minutes. The sessions are I prescribed once a day for six days a week. In the studies | conducted here, the patients learnt SKY before the end of the | first week. The Yoga teacher was trained at the Art-of-Living foundation. Subsequently the same teacher supervised SKY either daily for inpatients or at weekly intervals for the outpatients. The first study8 was an open clinical trial on 46 drug-free, consenting, hospital outpatients (22 males) with a diagnosis of DSM-IV dysthymic disorder9. After learning, they had to practice SKY everyday for half an hour and avoid any medication for three months. Regular practice was defined as three or more practice sessions each week. They were assessed on Hamilton Rating Scale for Depression (HRSD)10 and Clinical Global Impression (CGI)11 initially, at one and three months. Remission was defined as CGI score of 2 or less at both one and three month as well as absence of criterion symptoms that justified a diagnosis of dysthymia at these assessment points. Thirty-seven patients had regular SKY practice in the three-month trial period and 25(68%) remitted. A higher proportion of those practicing SKY regularly showing remission suggested a dose-response relation. No clinically significant side effect was noted during the trial period. The second study12 was a controlled trial in drug-free patients with DSM-IV major depressive disorder with melancholic features9. These patients were not treated for this episode and had not received ECT or antidepressants in the past six months. All scored 17 or more on the 17-item HRSD10. Patients (n=45; males=20) were hospitalized for four weeks and were randomly but equally assigned to receive ECT, imipramine or SKY. No other treatment was allowed during the study. Bilateral ECT on alternate days was used under anaesthetic modification. ECT was withheld if patients reached a HRSD score of 7 or less on two consecutive weekly assessments. Imipramine was used in a fixed dose of 150 mg per day orally at bedtime. SKY was initially taught as mentioned above. The sessions were practiced under supervision in the hospital six days a week. The depression severity was assessed before starting treatment and weekly thereafter for four weeks. Data on depression scales showed that ECT group responded best but the imipramine and SKY groups were comparable. The number of responders (total HRSD score less than 8) was 14, 11 and 10 respectively in ECT, imipramine and SKY groups. Major limitation of both these studies was lack of rater bias. In a more recent study13 therefore, we randomized 30 inpatients with major depressive disorder into two equal groups. One practiced SKY as in earlier studies. The other group however, received 'partial' SKY. This latter was similar to SKY except that the third part, rapid cyclical breathing, was replaced by normal breathing for the same period. Each group of patients practiced separately. Clinician who assessed the depression scores during the study too was blind to the treatment groups. During the trial period patients were not given any drugs except tablet lorazepam (upto 4 mg per day) or zopiclone (upto 7.5 mg/day) if they reported significant distress on account of insomnia. The two groups showed significant reductions in the depression scores. Responder was defined as one having 50% reductions in Beck Depression Inventory14 (BDI) scores. More patients in SKY group responded than partial SKY group although at trend worthy level of significance (p=0.058; OR=4.6; 95% CI=0.9-23).  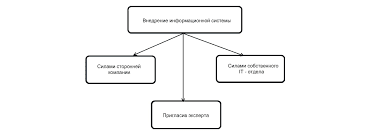 Что делает отдел по эксплуатации и сопровождению ИС? Отвечает за сохранность данных (расписания копирования, копирование и пр.)...  ЧТО ПРОИСХОДИТ ВО ВЗРОСЛОЙ ЖИЗНИ? Если вы все еще «неправильно» связаны с матерью, вы избегаете отделения и независимого взрослого существования...  ЧТО И КАК ПИСАЛИ О МОДЕ В ЖУРНАЛАХ НАЧАЛА XX ВЕКА Первый номер журнала «Аполлон» за 1909 г. начинался, по сути, с программного заявления редакции журнала...  Что способствует осуществлению желаний? Стопроцентная, непоколебимая уверенность в своем... Не нашли то, что искали? Воспользуйтесь поиском гугл на сайте:
|
 TREATING DEPRESSION USING SUDARSHAN KRIYA
TREATING DEPRESSION USING SUDARSHAN KRIYA